The morning of my shift involves setting up the following items:
(1) Anesthesia machine
(2) Airway setup
(3) Primary and secondary drug setup
ANESTHESIA MACHINE SET UP
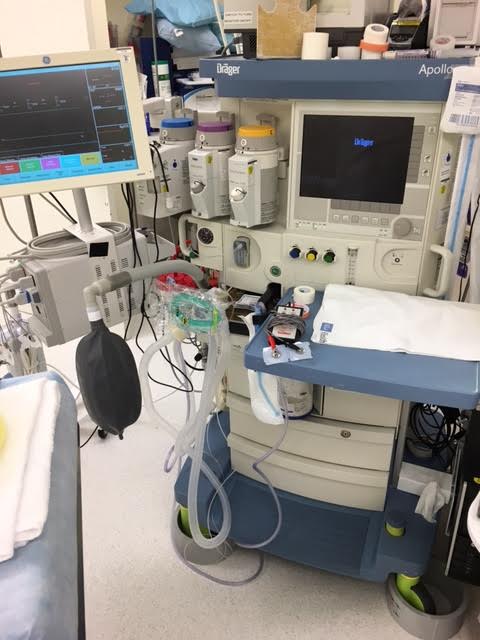
At my institution, we use an Apollo Drager anesthesia machine (among others, but for the purposes of this post, we’ll keep it simple and just focus on the Apollo Drager). The Apollo Drager is one of the newer machines out there and the set up is rather easy. It’s like an oversized iPad. I turned it on and push some buttons and it undergoes a series of tests in order to determine that all of the parts are working. Again, it’s much more complicated than this, but if you really want to know what goes into setting up an anesthesia machine, I’ll refer you to this video tutorial. Along with the anesthesia machine, I want to make sure I have access to a suction catheter and tubing in case my patient aspirates (i.e., vomits and inhales his/her vomitus) on induction (i.e., putting the patient to sleep). Additionally, I make sure the vital signs monitor is properly functioning because well, obviously, I want to be able to see my patient’s heart rate, oxygen saturation, respiration rate, temperature, and blood pressure during the procedure.
Apollo Drager Anesthesia Machine
AIRWAY SET UP
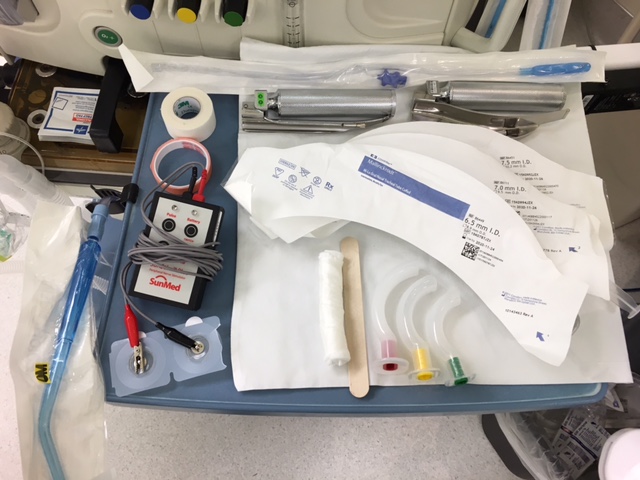
Clearly if a patient is to undergo surgery, you want to have an airway setup. In anesthesia, PREPARATION is key. Having a plan A, B, and C in place is critical if providing anesthesia to a patient. You want to be sure that you have the necessary tools and equipment nearby just in case you run into something untoward. A typical airway set up looks like this:
Typical Airway Setup
* Laryngoscope handle and blade (you need a tool to allow you to visualize where exactly you’ll be placing a breathing tube.
* 3 different sized endotracheal tubes (this is what you’ll be intubating your patient with and having tubes of various sizes readily available will prepare you just in case you come across a small airway and need a smaller tube)
* 3 different sized oropharyngeal airways (in case you run into issues with mask ventilating a patient, using an oropharyngeal airway will allow you to displace the patient’s tongue from obstructing his/her airway)
* Peripheral nerve stimulator (this tool allows you to assess the degree of paralysis your patient is experiencing; something that is important when you intubate)
* Tape and lots of it (you’ll use it to tape your patient’s eyes to protect them from corneal damage and you’ll need it to secure the endotracheal tube to the patient’s face because nothing’s worse than not being able to secure an airway)
PRIMARY DRUG SETUP
A basic drug set up looks like this:
In anesthesia, we’re concerned about 4 things: anxiolysis, amnesia, analgesia, and muscle relaxation. So, the following drugs are often drawn up for your typical case:
Midazolam (orange label) – to provide anxiolysis and amnesia
Fentanyl (blue label) – to provide analgesia
Lidocaine (white label) – to provide slight muscle relaxation particularly around the throat muscles and to help numb the vein that’s being infused (more on this later)
Propofol (Yellow label) – The drug that puts you to sleep; the Michael Jackson drug; the drug that has completely revolutionized anesthesia as it works fast and redistributes fast without any residual side effects (rather, with minimal residual side effects). Propofol often burns when it’s being infused into the vein, so we like to give lidocaine prior to giving Propofol to prevent the patient from experiencing any kind of discomfort.
Succinylcholine, Rocuronium, or Vecuronium (red label) – to provide paralysis; this is important if we decide to intubate our patients. You need the throat muscles to be completed relaxed so that the vocal cords are wide open so that you can insert the endotracheal tube and secure the patient’s airway.
SECONDARY DRUG SET UP
These are our back up medications that we have readily available in case of untoward situation occurs.
Phenylephrine and Ephedrine (purple labels) – these are medications to help keep the patient’s blood pressure elevated should you come across a lower than normal blood pressure reading.
Atropine (green label) – this medication helps to increase the patient’s heart rate if you come across a dangerously low heart rate.
Esmolol (brown label) – this medication helps to slow down the patient’s heart rate if you come across a higher than normal heart rate.
Usually, setting up the anesthesia machine, airway equipment and IV drugs takes about 10 minutes. Once I’m done with this setup, I go out to the preoperative unit, where I meet my patient and perform a preoperative evaluation.
Without getting into great detail as this forum is merely just a brief introduction into what exactly CRNAs do on a daily basis, the preoperative phase of case is about determining whether or not it is safe for the patient to proceed with his/her scheduled surgery. In essence, there are a set of pre-determined questions that should be asked of all patients and again, for the purposes of this post, we’ll just keep the discussion relegated to these questions. There’s a lot of nuance involved with performing a preoperative evaluation, but ultimately, you want to make sure that the patient’s heart and lungs can withstand the stress of surgery.